Why Healthcare Must Abandon the False Victory of a Compliance Culture
Healthcare does not keep losing ground for a lack of effort. It is failing because it has confused activity with progress—and compliance for control. Hospitals pass surveys. They meet regulatory thresholds. They report numbers and participate in an ever-expanding array of narrowly defined initiatives.
On paper, it looks like winning. But disciplined thought asks a harder question: If we are winning, why does it, in the end, always feel like losing?
Why does public trust erode as effort expands? Why do workforce shortages deepen despite constant recognition of the problem? Why do margins tighten even as organizations grow the care they can offer? Why do external forces increasingly dictate how care is delivered? Why do losses—clinical, financial, operational, and reputational—grow?
Because compliance—how healthcare measures quality in the bureaucratic quality culture where it stalled—is, by design, backwards-looking. It confirms that yesterday’s standards were met. Yet does too little to ensure readiness and control of what will emerge with tomorrow’s challenges—a future where every innovation and elevation in complexity introduces new risks and decision points that determine net gain versus net loss. And so, an uncomfortable truth keeps emerging: Beneath an industry capable of extraordinary, life-saving work lies a system that keeps steadily absorbing a compounding kind of loss. Not through dramatic failure-but through the accumulation of small, tolerated gaps in performance—financial losses, operational inefficiencies, and stories of preventable harm. Each one explained. Too many not prevented. Very few ever eliminated.
A Culture of Compliance
This is the signature of what Robert Westrum and Philip Hudson describe as a bureaucratic safety culture. Information flows-but slowly. Problems are acknowledged, but contained rather than solved. Success is defined by adherence-not outcomes. Activity expands-but never organizes into control. And over time, the wins that signal progress become harder to explain, as more resources that would have once been invested in future growth are instead consumed by efforts to survive the present and fix the past.
It is a loss not triggered by overt failure, but by a slow, insidious drift—what Jim Collins describes as a quiet erosion in the absence of discipline—where visible signs of progress mask an underlying reality of decline. Given enough time, undisciplined activity, and accumulated loss, that drift becomes decisive. Some organizations fail outright. Others do not fail—but fade, capitulating to eventual irrelevance as they are outperformed by new entrants into the marketplace who are unburdened by the cost, complexity, and accumulated losses that bureaucracy sustains.
In the end, the pattern is unforgiving. When activity replaces discipline, compliance substitutes for control, and complexity is mistaken for competence, decline is not merely possible—it becomes the trajectory of a hospital’s future.
This is a culture that aligns, uncomfortably well, with what Jim Collins describes in How the Mighty Fall: not outright failure, but the slow, insidious erosion of success masked by visible signs of progress.
A Flawed Economic Assumption
From its early rise, modern healthcare operated on a premise few industries could sustain: that cost, by virtue of purpose, justified itself. If the work saved lives, the price was secondary—whatever it might be. And for a time, that premise held. Not because it was right, but because the system could absorb the strain.
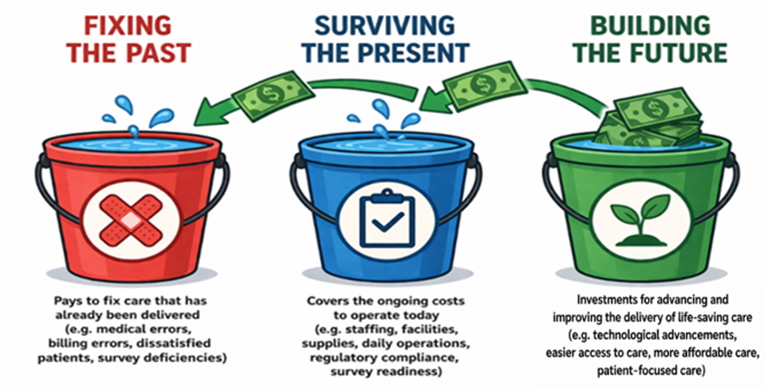
Hospitals expanded resource-intensive activities without much concern for cost and labeled it progress. Spending to the “100”—fixing problems after the fact—became standard practice. Waste was not corrected; it was financed. A steady influx of new dollars masked inefficiency. Even patient frustration was dismissed— reframed as ingratitude rather than being recognized as an important signal of decline. The system never confronted a simple truth: What works in abundance rarely survives under constraint.
As healthcare advanced—delivering more care, extending more lives—it also grew more tolerant of what was suboptimal. Payment models lagged reality and rewarded undisciplined behavior. Regulations calcified instead of evolving. What should have integrated fragmented. Costs rose. Access tightened. And quality—rather than emerging as a clear standard of excellence—devolved into compliance with yesterday’s measures.
Incentives drifted out of alignment. External pressures intensified. Complexity compounded. Frustration became embedded in the system. What should have functioned as an interdependent ecosystem—caregivers, payers, and public stewards—devolved into a web of strained relationships. Negotiation replaced collaboration. Compliance replaced purpose. The system became adversarial, transactional, and distracted—ceding control outward while constructing an increasingly fragile house of cards. Fostering an environment where organizations do not fail all at once. They erode—quietly, steadily—by consuming the future to survive in the present.
The result is an industry no longer fully in command of its own work. Public confidence has fallen—from roughly 85% to near 30%. The operating environment feels less like a coordinated system and more like a fibrillating heart: constant motion, diminishing control. Bureaucracy without vitality.
The Defining Choice
As reimbursement tightens and margins erode, healthcare providers face a defining choice: to build a flywheel, as Jim Collins describes—focused on forward momentum—or to remain trapped in a doom loop characterized by narratives of perpetual decline.
This is not a question of tactics. It is a question of discipline. It is a choice between, on one side, a renewed commitment to achieving a generative culture of quality—one that systematically protects and allocates resources to promote future growth: innovation, capability, financial strength, and patient loyalty. A system that builds momentum over time. One that invests not in fixing what chance failed to control for yesterday, but in creating a stronger tomorrow through disciplined control of what matters.
Or, on the other side, a choice to perpetuate a pattern of decline—fostered by the false victories of a bureaucratic culture—where an increasing share of resources is consumed by a focus on stabilization. Not to create, but to correct. Not to advance, but to sustain. Not to lead, but to follow.
It is a choice between a path forward that requires a fundamental realignment—something Jim Collins describes as renewal and recovery. One in which quality and economics are not competing priorities, but inseparable forces that reinforce one another in service of long-term strength—or—the continuation of a system that, bit by bit, draws from what should fuel the future to satisfy the present. Resources shift toward patching the past. Effort fragments across compliance-driven definitions of “quality,” drifting further from the outcomes that could restore organizational health, as momentum stalls and energy dissipates.
The defining decision is this: to rebalance and regain control—or to continue down a path where the core issue is not financial constraint, but a lack of discipline.
Understanding the “Doom Loop”
To understand why efforts in healthcare fail to produce projected results, one must see the doom loop embedded in how the industry operates. How today slowly and insidiously consumes tomorrow.
Healthcare fails to be in control of the risks that frustrate patients and threatens business health. Medical errors occur, costs escalate, billing errors multiply, wait times get longer, communication gets harder, care seems increasingly dismissive, continuity fractures, and patient frustrations build-causing patients to look outside traditional patient-provider relationships for answers.
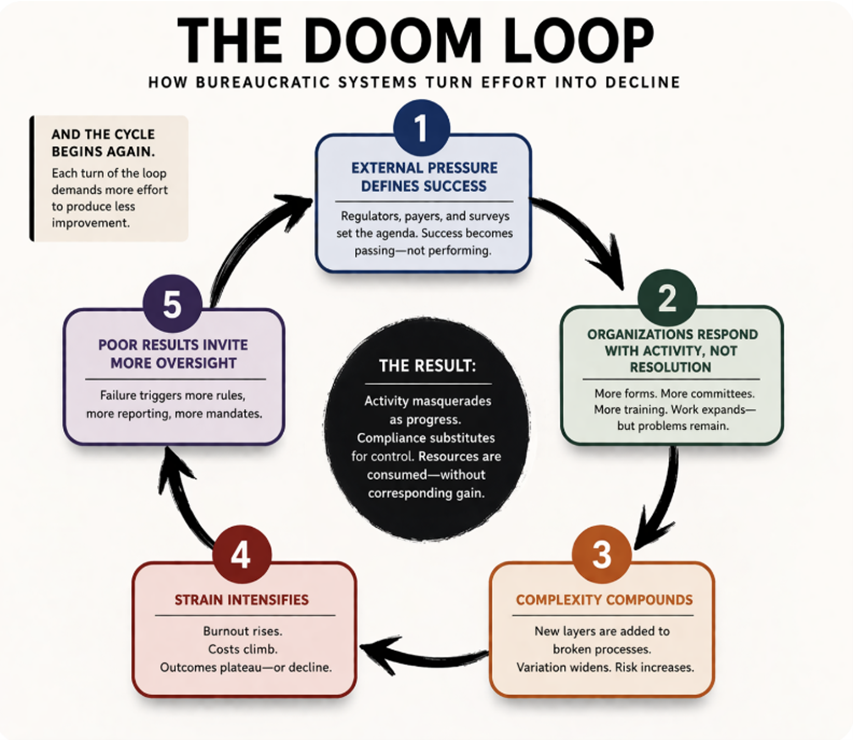
1. External pressure, rather than internal goals, defines success.
Regulators, payers, and surveys set the agenda. Success is defined as passing-not striving for optimal performance.
2. Organizations respond with activity, not resolution.
More forms, More committees. More training. More spending to the “100.” Work expands—but problems remain—too frequently getting bigger and more costly.
3. Complexity compounds.
New layers are added to broken processes. Variation widens. Risk Increases.
4. Strain intensifies.
Burnout rises. Costs climb. Outcomes plateau—or decline.
5. Poor results in the absence of disciplined control invite more oversight.
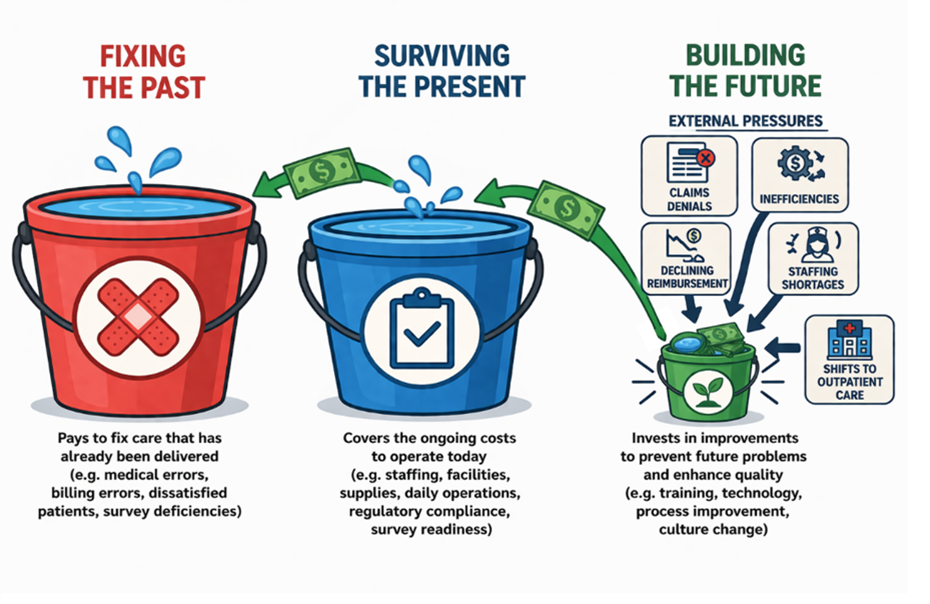
New risks—along with the repetition of old risks—trigger more rules, more reporting, more mandates, and more financial consequences. More spending in the buckets for fixing the past and surviving the present at the expense of what is left over for future funding.
And the cycle begins again—taking healthcare farther and farther from its desired goals.
This is the doom loop healthcare has long believed it was immune to: activity mistaken for progress, compliance mistaken for control, and resources consumed with no corresponding gain. With each turn of the loop, more effort is required to produce less.
This is not a failure of intent. It is a failure of trajectory. Resources are relentlessly pulled toward patching yesterday and surviving today’s demands. Investment in future capabilities is squeezed, quarter by quarter, until the organization begins to hollow out from within. Quality becomes something to report rather than achieve. Compliance displaces commitment. Metrics multiply, but meaning erodes—all while the system keeps moving, not with momentum, but merely with motion.
At its core sits a flawed design: the belief that financial strength comes from chasing new money rather than exercising disciplined control over the money already in hand. In a bureaucratic quality culture, it becomes entirely possible to spend $300,000 to create the appearance of progress—and end up exactly where you started, or worse, further along in the doom loop. Not because the solution is unknowable, but because, when the moment demands it, the system resists the very changes that would unlock the savings and success that today’s leaders seek.
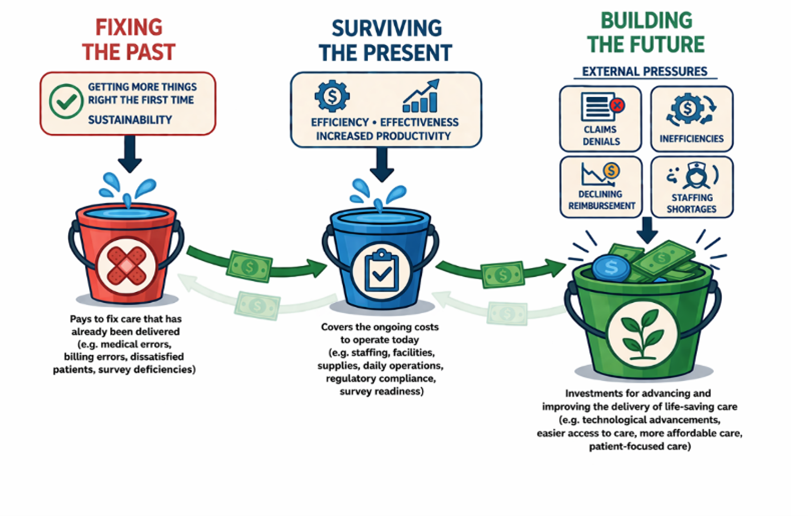
Contrast this with a generative culture, where a single $300,000 investment—paired with a commitment to greater efficiency, effectiveness, resilience, and disciplined systematization—could produce $1.2 to $1.9 million in initial savings. Not as a one-time gain, but as the first push in the flywheel Jim Collins describes. With disciplined systematization, the next turn of the wheel can free $3 million or more, shifting resources away from survival, rework, and fixing the past—and back toward building the future.
No silver bullets are needed. No breakthrough technology is required. Just disciplined control, smarter allocation, and better decisions—repeated consistently over time. That is how the flywheel begins to turn.
The Flywheel
In sharp contrast to the backward pull of the doom loop, the flywheel—as described by Jim Collins in Good to Great—represents how enduring organizations build strength: quietly and steadily, through disciplined and consistent action. There is no single defining moment. No breakthrough event. Only the cumulative effect of doing the right things, in the right way, over and over again.
In healthcare, the flywheel takes shape through quality and risk management practices that do more than react to yesterday’s failures—they systematically reduce the likelihood of their return. The focus expands beyond regulatory compliance to full organizational control: clinical, financial, operational, and reputational. It is a system unafraid to embrace change—especially when change leads to greater success.
The shift is fundamental: from recovery to prevention. From fixing what broke to ensuring that it does not break again. From spending to “100” after the fact to maximizing how every dollar is spent. Each turn of the wheel brings prior risks under control while preparing for what comes next. Over time, effort compounds. Less energy is spent repairing the past. More capacity is directed toward building what will advance the delivery of care.
This is not about intensity. It is about consistency. Discipline builds systems. Systems build trust. Trust strengthens relationships—within the workforce and with the public. Momentum follows. What once required constant correction becomes increasingly stable. What once demanded reaction becomes governed by control. And what once consumed resources begins to generate them.
That is how the flywheel turns—not by force, but by consistency. In healthcare, it can begin with a single shift:
From reacting to requirements to controlling the systems that produce results.
And then it builds:
Getting more right the first time—in increasingly efficient, effective, and sustainable ways—reduces work.
Reducing work → frees capacity.
Freed capacity → improves focus and performance.
Improved performance and capacity → strengthen outcomes and economics.
Stronger outcomes → reinforce trust, satisfaction, and stability.
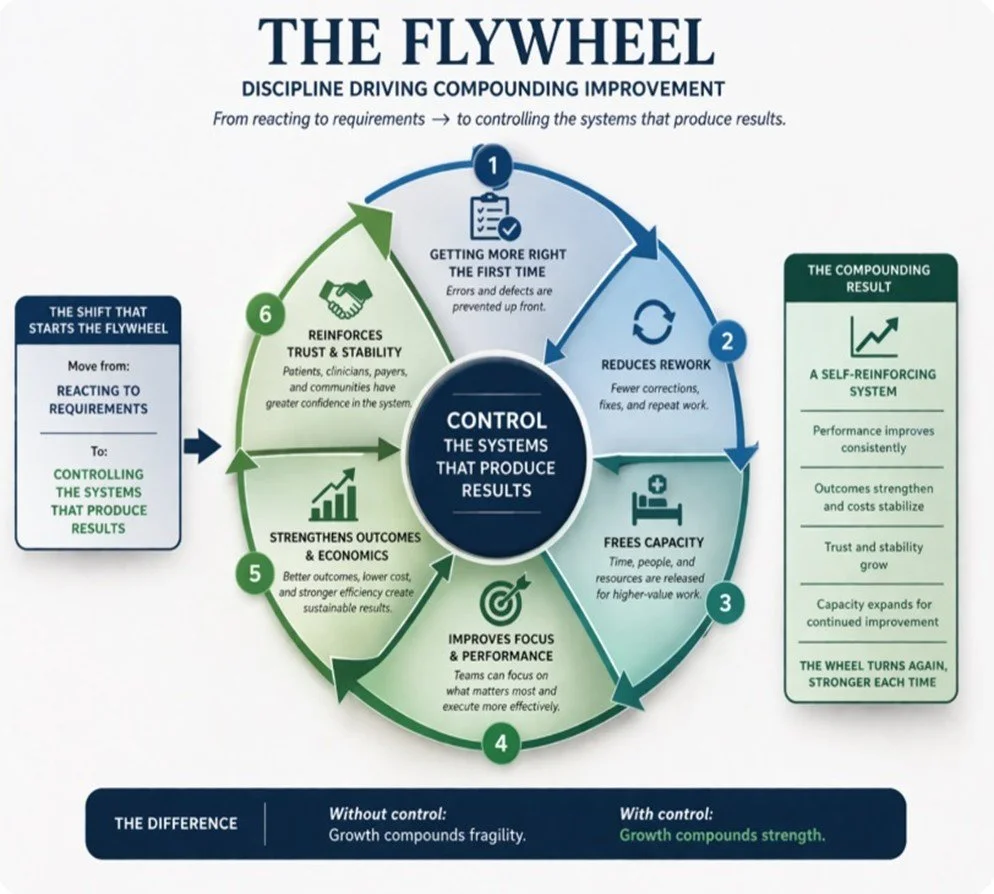
And the wheel turns again and again—slowly and steadily—moving the industry from where it is today to a place where stronger clinical, financial, operational, and reputational outcomes can naturally occur.
It reflects a fundamental rule: without control, growth compounds fragility. But with control, growth compounds strength.
Making It Real
The most important question in healthcare is no longer theoretical: How many more bureaucratic moves—turns of the doom loop—can healthcare afford to survive, when the evidence of its decline is no longer arguable?
Consider the adoption of electronic health records. Introduced with the promise of progress, they have, in too many ways, delivered the opposite: downward pressure on operating margins, growing workforce burnout, fractured clinical communication, new categories of error, little control over past risks, and rising patient dissatisfaction—as caregivers spend more time documenting than caring.
Not because the technological concept itself is flawed, but because today’s tools were built to solve yesterday’s requirements—without the structural discipline to control what tomorrow may demand. In doing so, they reinforce the defining behavior of a bureaucratic culture: when something breaks, it is not fixed—it is layered over. Creating increasingly costly and complex maintenance. More add-ons. More workarounds. More rework, inefficiencies, and unintended consequences. More stress on the workforce. More dissatisfaction among patients. All of it funneling greater sums of money and manpower into the same two buckets that bureaucratic quality cultures treat as inconsequential: fixing the past and surviving the present—while the third bucket, growing the future, quietly starves.
Not because of what vendors built, but because of what healthcare chose to prioritize—chasing more rather than ensuring the creation of tools that deliver control. Control needed to build a stronger future in an increasingly demanding environment. As a result, a costly investment that should have delivered efficiency, effectiveness, productivity, error reduction, and timely access to well-organized patient information has, in many ways, produced something weaker than the industry’s traditional manual approaches.
This is how decline becomes visible in a compliance culture. Technologies meant to improve care introduce new burdens because they are designed to achieve conformance—not breakthrough performance. Documentation expands while human connection contracts. Costs rise while productivity stalls. New errors emerge as old ones persist. Not by accident, but as the predictable outcome of a system focused on compliance—not control.
Then because few are willing to fix what is truly broken in the aftermath of massive expenditures—often funded by billions in taxpayer dollars—the pattern of decline continues. Incrementalism prevails. Band-Aids grow larger. Activity expands. Initiatives multiply. Spending increases. Frustration deepens. Resources are depleted. The system itself grows weaker, not stronger—all while leaders cling to the hope that relief will come from one more investment, one more expansion, one more service—built on projections the system is not designed to deliver.
And beneath it all, the machinery of bureaucracy expands—quietly and persistently—redirecting time, talent, and capital into activities that sustain the system but do not strengthen it. Setting the stage for a deeper descent into the doom loop, where more is done, more is spent—but less of what truly matters is achieved.
The Hidden Consequences
Producing consequences that are no longer abstract—becoming more visible and increasingly palpable every day. Something demonstrated in the reality of Never Events: failures that should not happen—occurring when the capability to prevent them exists but is not exercised. Adding to the growing frustration of the American people and the ongoing decline of the healthcare industry—bringing more complexity, more confusion, and more strain to the patient-provider relationship.
Compounded by a new kind of externally imposed loss—one that depletes funds that once flowed into the bucket for investing in the future, while simultaneously increasing expenditures in the two buckets dedicated to surviving the present and fixing the past. And no matter how much discussion there is about escalating costs and the power of prevention, the response from healthcare too often defaults to costly compliance rather than effective control—passing surveys and meeting regulatory requirements through minimal adherence to process-oriented standards that do not have to produce meaningful results, even as the consequences of multi-resistant organisms continue to grow.
Thus, these dangerous infections are not only increasing—they are becoming more lethal. Costs are climbing. Risks are compounding. Frustration is building. The trajectory is unmistakable: the cost of treating these infections could increase tenfold or more in the near future. Yet the industry, failing to act in its own self-interest, does not correct course. Instead, it reallocates more of its scarce resources—not out of necessity, but by design—into the same buckets for fixing the past and surviving the present while watching its bucket for funding the future decline.
Choosing to remain settled in the rhythm of bureaucratic compliance where processes multiply. Work expands. Time is consumed. Value is defined not by net outcomes, but by the visible presence of survey-satisfying activity. A system that rewards motion over progress while the public, in turn, grows weary—asked to fund a model that markets safety through compliance, often at its lowest acceptable threshold. Dismissing the way trust erodes. And as trust declines, payers and regulators respond not with simplification, but with escalation—shifting the rising costs of largely preventable outcomes away from patients and themselves and onto providers who choose a doom loop over a flywheel.
Learning from the Pattern
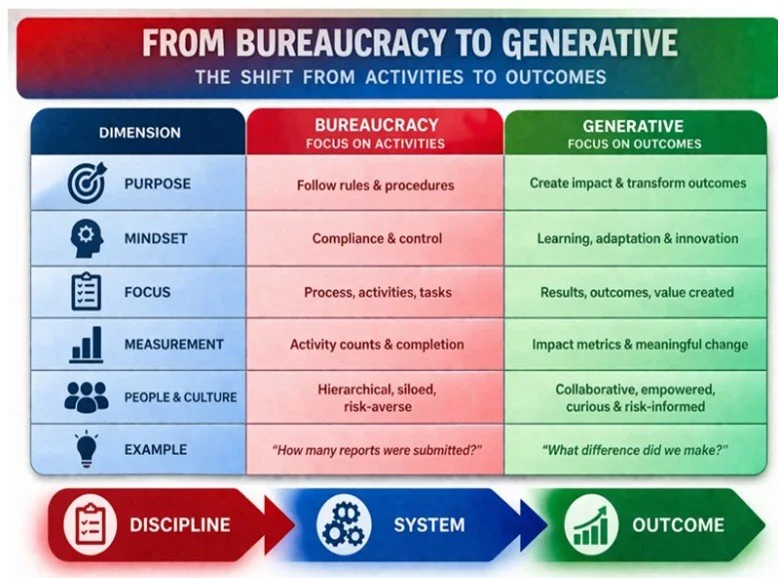
In a bureaucratic culture, efforts are fragmented. Leaders meet. Committees discuss. Initiatives launch—and can persist indefinitely without results. Process-oriented measures are satisfied, but the system that produces them remains fundamentally unchanged.
This is revealed in the way work multiplies. Processes duplicate. Steps expand. Silos grow in number and size. Time is consumed. Value, in the eyes of the customer, declines. As when compliance becomes the objective, the entire frame of thinking shifts. The questions are no longer anchored in impact—Does it work? Did we make a difference?
Instead, they drift toward optics and defensibility—Can we document activity? Can we demonstrate adherence? And in that quiet shift, substance yields to appearance:
Did we review antibiotic use—even as resistant organisms continue their steady rise and preventable infections persist?
Did we achieve strong patient satisfaction scores—even as trust, in any meaningful sense, remains unchanged or declines?
Did we pass the external audit—even if it offered little insight into the risks gathering just beyond the horizon?
Did we excel in accreditation—even though, days later, a preventable, life-threatening error could still occur?
Gradually, almost imperceptibly, complexity expands and control erodes. Layer upon layer of activity accumulates. Busywork aimed at yesterday’s problems grows until it consumes the very capacity needed to make tomorrow better. A design that measures activity to produce more activity—a system that measures compliance only to require more compliance. And decline perpetually occurs through the accumulation of tolerated inefficiencies, wasteful costs, and avoidable losses—explained, managed, but rarely eliminated.
And this is the subtle danger that hides in a bureaucratic quality culture: when the scoreboard replaces the mission, success becomes something we can report rather than something we can feel in outcomes that truly improve. Activity becomes evidence, and evidence becomes a substitute for effectiveness. Systems measure themselves by what they can prove against yesterday’s standards rather than by what they have improved to make tomorrow better—more efficient, more effective, more resilient, and more in control of what causes harm.
The Shift That Matters
Healthcare did not get here over night. As medicine expanded its technological frontier, it gained extraordinary capability—advanced diagnostics, powerful drugs, complex surgical interventions. These breakthroughs saved lives, but they also introduced new forms of risk. Care became more effective—and at the same time, more dangerous. More expensive and more complex.
Systems became more capable—and more fragile. Revenues increased—but so did expenses. And in the widening gap, a dangerous set of beliefs quietly took root. Costs were rationalized, not rigorously controlled. Complexity was individualized, not systematized and managed. Errors were absorbed into the daily flow of care, becoming routine, not intolerable. Failures were explained away—rarely redesigned out of existence.
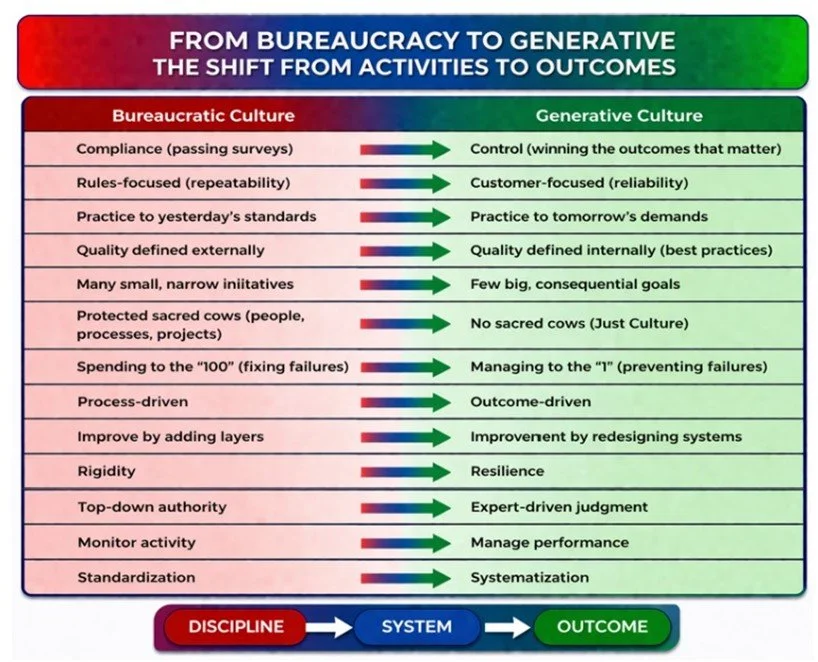
Leaders blamed careless and irresponsible people. Clinicians pointed to oddities in patients. And the concerns of the American public were dismissed as ingratitude for what the system could provide. All the while, the system itself—the very architecture producing these outcomes—remained largely untouched. Simply growing in size and compliance dictated obligations. And within the tension created, healthcare’s decline became easier to see. What Westrum and Hudson describe as the failure to migrate from a bureaucratic culture defined by activity to a generative culture defined by outcomes. What Collins would recognize as the evolution to a more disciplined system—where quality and economics are not competing priorities, but inseparable for the outcomes to be achieved. Something that James Reason framed as holding the line between innovation and safety.
Different explanations—but the same principle. An understanding that systems produce exactly what they are designed to produce—clinically, financially, operationally and reputationally. Dysfunction—or control. Errors—or optimal outcomes. Waste—or wise investment. Failure—or success. There is no neutrality. And without the kind of quality that delivers control, performance is left to chance.
So as long as healthcare remains anchored in a bureaucratic quality culture where it tries to sell compliance as a measure of safety, the pattern is predictable: more rules, more reporting, more initiatives, more survey standards, more externally-driven consequences, more costs, more penalties and more resources flowing into buckets for fixing the past and surviving the present. And less—every year—available for funding the future in an environment where the goal of the American people is the same as for any other product they buy—optimal care that meets their needs at an affordable price.
The Real Choice
The real choice for healthcare now is not what it appears to be:
Not whether to chase more technology and services.
Not autonomy versus control.
Not growth versus quality.
Not compliance versus discipline.
It is something far more fundamental to survival—the shift from bureaucracy to generative systems, from compliance to control—in an environment where every new bureaucratic solution becomes just another input into the same equation: more cost, more activity, and less achieved.
This is not an isolated pattern—it is systemic, as long as healthcare continues to operate as if it can spend its way out of its problems. Chasing more while quietly accumulating larger losses in the same two places: repeatedly fixing the past and inefficiently surviving the present. Exactly as Collins describes it—the undisciplined pursuit of more, producing diminishing returns. The appearance of progress outpacing the reality of success. A gap between what is achieved and what is needed that continues to widen—not because the goal is wrong, but because the system, as designed, cannot deliver.
This choice is not theoretical—it is being made every day, including now, as the industry considers how to deploy the $50 billion investment from the American people through the Rural Transformation Program. A taxpayer-funded effort to sustain rural healthcare providers—where the key word is not funding, but transformation.
The risk is not whether the money will be spent—but how. Will it fund true transformation—the kind of change that strengthens rural providers in ways that are meaningful and durable enough to survive an increasingly challenging environment? Or will it follow a familiar pattern: fragmented initiatives, incremental fixes, expanding processes, more bureaucracy, more metrics to report, more debt—more activity that signals motion, but not forward progress?
Exercising the signature moves of a bureaucratic culture: Motion without growth. Process without outcome. Cost without control. Externally driven projects without internally driven goals that are big enough to matter.
Which leads to the only question that ultimately matters: When the money is gone—what will remain?
Stronger providers:
More efficient
More effective
More resilient
More in control of their futures—capable of surviving and competing in a more demanding world
A stronger healthcare safety net for the American people
—or—
Providers fundamentally unchanged:
Still fragile
Still dependent
More in debt
Still hoping for another infusion to stay afloat
Will we strengthen rural healthcare—or expand the size of our healthcare deserts? That is the real choice. And it will not be decided by intention, but by action.
Because in the end, the constraint is not resources.
It is the discipline to create something better than what exists today.
It is the system of control required to sustain it.
It is the willingness to think beyond the immediate and build for what comes next.
And, nowhere are these choices more consequential than in rural healthcare. What has been lost is not just margin or staffing—it is the power, influence, earning potential, and, perhaps most critically, the goodwill required to survive. The question is whether the industry is willing to restore them—or simply create the illusion of effort.
Final Thoughts
The real question today is not whether healthcare is working hard enough. It is whether that effort is translating into forward motion—or quietly compounding into backward-leaning exhaustion. Because effort, by itself, is never the differentiator. Direction is.
Today, too much of the healthcare system is designed to pull resources into two counterproductive wells: fixing the past and surviving the present. And the longer that pull goes unchallenged by effective answers, the more inevitable demise begins to feel.
But it is not inevitable. It is a choice. A choice to slow the steady migration of time, talent, and capital into yesterday’s problems and today’s urgencies. A choice to reclaim and redirect the resources already there—hidden in plain sight, but chronically overcommitted. A choice to build again, rather than simply sustain.
Because in the end, the system will move. The only question is whether it moves forward by design—or drifts backward by default.
Each of my posts builds on the previous ones to better clarify why healthcare is struggling. If you haven’t already, I recommend reading my last two posts. Click here to access the previous posts.
No More Grasping for Salvation: Why Healthcare Must Start Managing Money and Quality as Two Sides of the Same Coin (March 26, 2026)
Unlocking Healthcare Excellence: How to Fix the System from Within (March 2, 2026)