Why Healthcare Must Start Managing Money and Quality as Two Sides of the Same Coin
Why does logic suggest the American healthcare industry should be thriving—yet the reality tells a very different story? From the outside, healthcare looks enormously successful. Massive hospital systems dominate our skylines. Revenues run into the billions. Scientific and technological breakthroughs continue at an extraordinary pace.
Yet behind that impressive façade, many healthcare providers are slowly and insidiously dying in a self-perpetuating doom loop. Operating margins keep shrinking. Workforce shortages are worsening. External oversight and demands continue to grow while public frustration is rising. Making the possibility of closure—or at best, capitulation to competitive irrelevance—no longer theoretical.

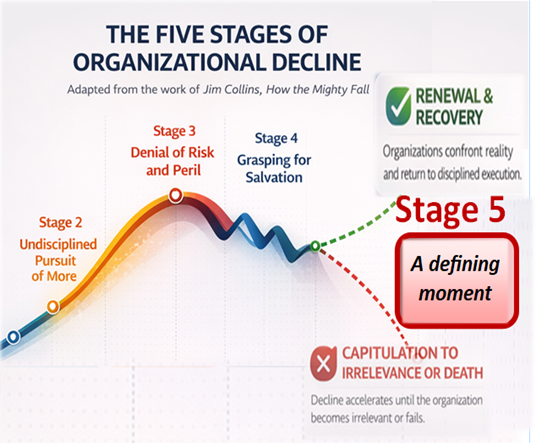
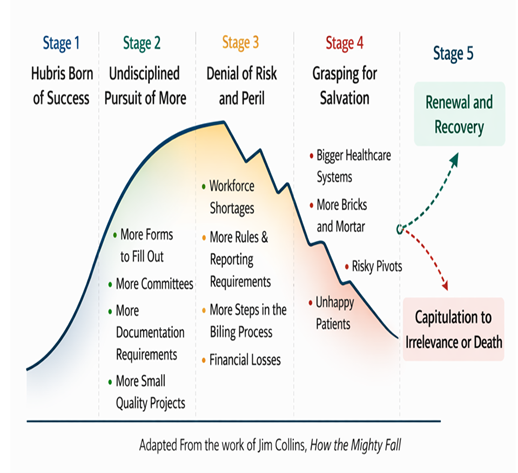
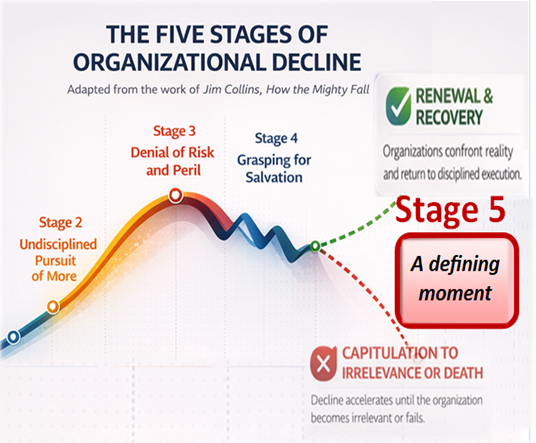
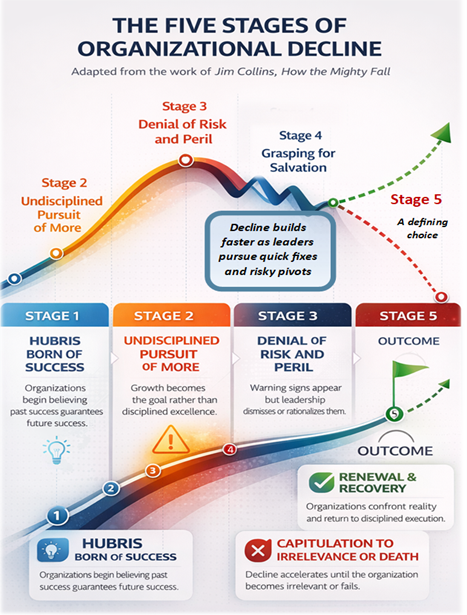
In this post, we will continue to explore how an industry capable of saving lives and advancing medical science finds itself where it is today. Looking through the useful lens of Jim Collins’ works about How the Mighty Fall, we will compare the uncomfortable trajectory of American healthcare to what he explains as the demise of once successful and powerful businesses as they pass through five predictable stages of decline—stories of failure that evolve when leaders cling to what they want to believe instead of confronting uncomfortable realities.
A Decline Decades in the Making
Healthcare’s current challenges didn’t appear overnight. They began during the early years of medicine’s technological revolution. New diagnostic tools, drugs, and surgical techniques dramatically expanded what clinicians could do and the money to be made. Breakthroughs producing one of the greatest scientific transformations in modern history—while introducing choices that would bring healthcare to where it is today.
Advances in what it could offer the American people that came with an insidiously dangerous shift in mindset where many within the industry began to assume that clinical innovation alone would sustain public trust and grow the industry’s wealth and power. Far less attention was paid to how care was delivered, how errors were managed, or how costs were escalating—all at a time when financial modeling reinforced a hubris type of thinking.
Healthcare organizations were reimbursed largely based on what they claimed it cost to deliver care. Errors and complications often generated additional billable services. Meanwhile, strong patient loyalty and limited external oversight allowed providers considerable autonomy in how they interpreted the world they managed.
Growth became the dominant priority. And for a while, it worked until the long-term consequences started to appear. Public confidence in healthcare institutions—once near 85% in the mid-1960s started to decline—falling to roughly 30% today. Operating margins became increasingly fragile, and burnout started pushing operationally important clinicians out of the environment.
Creating an industry that had everything going for it but kept expanding faster than its operational discipline could control for—paying the price in the predictable pattern of decline that Jim Collins warns about.
When Healthcare Opened the Door to Outsiders
As costs rose, safety failures became more visible, and the industry’s hubris rationalized it all, frustration grew among patients and policymakers. Gradually opening the doors to new actors whose influence would start reshaping how healthcare operates. Regulators, accreditation surveyors, and insurance payers set the stage for an ever-growing group of market players that once only operated on the periphery of healthcare delivery to play an increasingly influential role in how care is structured, measured, and reimbursed.
Ironically, shifting an industry that was enjoying tremendous power, influence, earning potential, and goodwill into one that now isn’t—all because it failed to regulate its growth effectively. Prioritizing scale over quality and unintentionally inviting outsiders to fill the vacuum it left behind.
The “More” Syndrome
Jim Collins describes one of the most dangerous stages of decline for successful businesses as the “undisciplined pursuit of more.” Like many, healthcare organizations began to believe that growth itself was the solution to long-term success. More facilities, more technology, more service lines, and more acquisitions.
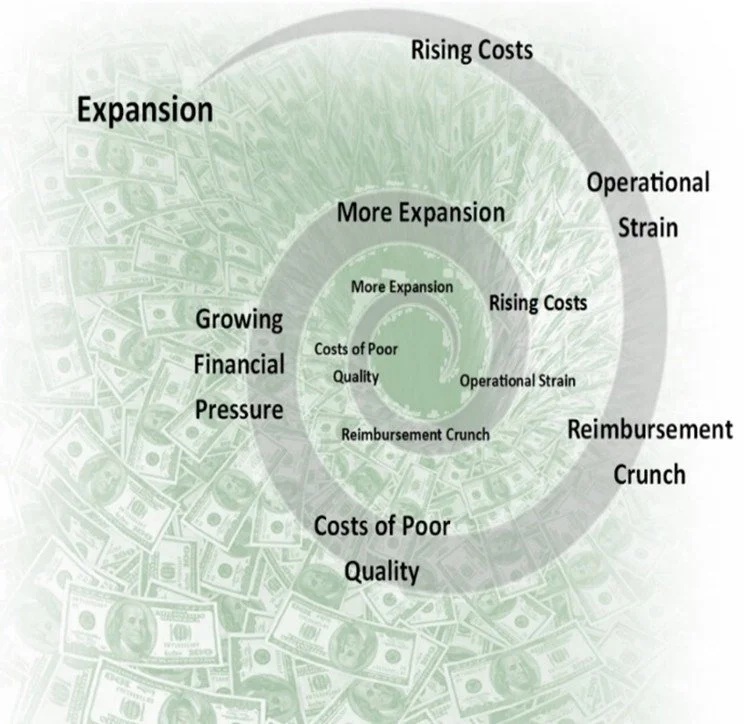
A pattern of self-destructive behavior that healthcare has embraced for too many decades-expansion without operational discipline-creating a dangerous misconception about what might be called the illusion of saving. When organizations reduce investments in safety systems, workforce development, or operational infrastructure, it may look like cost control when in reality, it simply defers the consequences of much larger costs and losses into the future. Feeding the slow and insidious decline of the business. Something that Hewlett-Packard co-founder Dave Packard warned about decades ago:
No company can consistently grow revenues faster than its ability to attract and retain the people needed to sustain that growth.
Yet too many in healthcare did just the opposite—pursuing scale without building the operational foundation—the people, systems, and culture—required to sustain it.
Denial of Risk and Peril
Healthcare has too often ignored, discounted, or rationalized the warning signs of trouble while performing just well enough to avoid confronting them. Meanwhile, the power, influence, earning potential, and public goodwill once enjoyed have steadily eroded. Negative data is explained away, the benefits of life-saving care are amplified to deflect scrutiny, blame is externalized, debate is muted, and the system continues “fiddling while Rome slowly burns.”
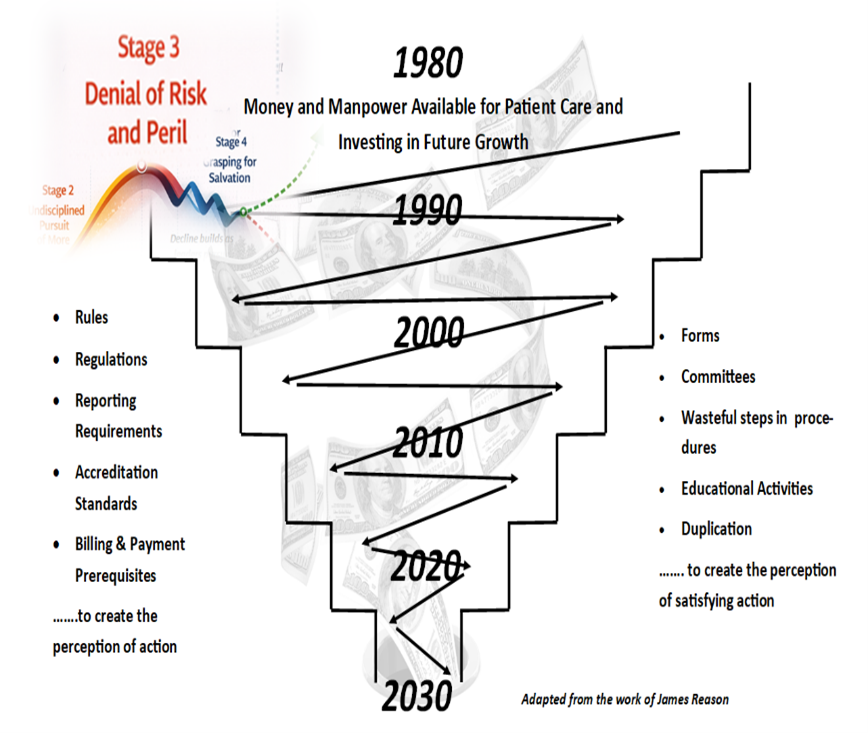
Quality improvement that devolved into a resource-consumptive game of tit for tat: doing just enough to satisfy the latest demands from an expanding network of external authorities. Success is measured by minimal compliance and a dangerous illusion of savings rather than genuine financial, operational, or reputational strength—with little concern for the impact on patient care and frontline caregivers. Resulting in a slow, self-reinforcing cycle of decline that leaves the public reliant on ever more rules, regulations, survey standards, and oversight—substitutes for the discipline the industry has failed to sustain internally.
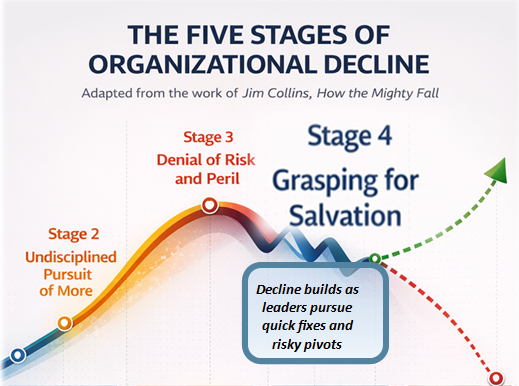
Grasping for Salvation
Today, too many healthcare providers appear to be sinking fast in what Collins calls “grasping for salvation.” The stage where leaders are driven by impatience and the desire for quick wins while continuing to cling to the undisciplined pursuit of more. Searching for silver bullets—simple, rapid solutions to fix complex, chronic, and high-stake problems.
• New technologies
• Mergers and acquisitions
• Geographic expansion
• New service lines
Common strategies that can create value when done thoughtfully, but in healthcare too commonly do just the opposite when used to avoid confronting deeper operational problems. Simply reinforcing the industry’s cycle of decline that has turned into a fifty-year-old doom loop.
A story of perpetual deterioration where across the country, the consequences are increasingly visible.
· Rural hospitals are closing, creating healthcare deserts.
· Mid-sized hospitals struggle to stay financially competitive.
· Even large systems are now having serious conversations about long-term sustainability—struggling to manage the behemoth healthcare systems they have created on an assumption that size would protect them.
And too often, the entrenched response to financial stress only deepens the problem as the next solution is more of the same, not fixing what’s broken. Like what happened to one struggling hospital that hired a new CEO whose first major decision was to purchase an expensive MRI machine to boost revenue. But because the hospital’s real problem wasn’t a lack of technology but was a reputation for poor service and medical errors that had driven patients away, the problem he was hired to fix was not solved with a very expensive shiny new machine. Another expensive asset that exacerbated the financial pressures he was hired to solve, especially when there was no plan for the real problems that haunted hospital-patient loyalty.
The Real Solution
Healthcare’s challenges will not be solved by another wave of expansion, reporting more numbers, the creation of more administrative positions, more bureaucracy, and rearranging the deck chairs on a floundering ship. They will be solved by rediscovering something far more fundamental. The fact that quality and financial performance are inseparable. They are not competing priorities. They are two sides of the same coin.
How well an organization delivers and manages care—or manages quality—ultimately determines:
• How efficiently resources are used.
• How productive clinicians can be.
• How much trust patients place in the system.
• How much spending to the “100” in the 1:10:100 Rule eats at the bottom line.
• How easy it is to achieve advancements in patient care.
• And how financially sustainable the organization becomes.
High-performing industries understand this relationship while healthcare too often behaves as if it does not.
The Choice Ahead
Healthcare now faces a defining moment.
Continue chasing growth—building more facilities, buying more technology, and hoping scale will eventually solve its problem—or embrace what Collins describes as renewal and recovery.
Renewal—something that doesn’t present itself as a cure-all or a sweeping panacea. Instead, it emerges through something far less glamorous—but far more powerful: the disciplined rebuilding of the systems that determine performance.
• Operational efficiency and effectiveness
• Workforce investment and growth
• Proactive risk management
• Strong patient-provider relationships
• Relentless focus on quality—getting it right the first time in the most business- supportive ways
Revitalizing an industry once capable of extraordinary innovation—now fighting not for progress, but for survival. Reclaiming the essential truth that financial discipline and quality are not opposing forces, but twin engines of greatness. Breaking free from the downward spiral Jim Collins warned of, in which—if unchecked—no scale, good intention, or legacy will be enough to save our institutions.
Only disciplined management of both money and quality will.
Capitulating to irrelevance or Death.
The real question is simple: Will healthcare continue grasping for salvation, or finally learn to manage both sides of the coin it relentlessly chases?
And if it refuses, how many of our providers will perish, not by choice—but by replacement. Not by revolution from within or policymakers, but by competitors with their own vested interests in stronger healthcare delivery unencumbered by the assumptions and entrenched practices that paralyze traditional healthcare.
Companies like Walmart and Amazon who are already experimenting in the very trial-and-error phase Jim Collins describes—where early failures are inevitable, misunderstood, and often dismissed by current providers eager to believe the threat is overstated.
The final step where the greatest risk for healthcare is to read too much into early missteps while continuing to look outward for sympathy as it engages in hubris-driven practices. Doing more of the same while emerging players look for something else entirely: a better way to deliver care that is more accessible, more affordable, and far less prone to error—the very things Americans are finding increasingly difficult to obtain from the system that was originally built to serve them.
Recognizing the Frameworks of Strategic Failure
Across the country, hospitals are repeating a small number of predictable strategic mistakes. These patterns form its recognizable framework of decline.
1. The Silver Bullet Strategy
A struggling organization bets its future on a single expensive technology or service.
Example:
A financially distressed hospital purchases an expensive MRI machine—even though the patient volume, if honestly projected, could never generate enough revenue to cover the cost.
The logic is seductive……. This technology will save us.
But technology rarely saves organizations with broken fundamentals. When a hospital has a reputation for poor service or medical errors that keep patients away, the solution is not more equipment. It is rebuilding public trust.
2. The “If You Build It” Trap
Hospitals invest heavily in large capital projects based on the assumption that demand will follow.
Example:
A hospital builds a beautiful new addition without a realistic financial plan that had it managing money and quality like they are two sides of the same coin. At the time of opening, financial pressure prompted a hiring freeze for nurses—creating the first devastating blow to patient volumes. Compounded by the fast-acting, short-term fix of cutting physicians—the very professionals who generate the revenue that sustains the organization.
The result is predictable:
· Higher fixed cost
· Lower earning capacity
· Greater community dissatisfaction
· Lower morale
· Higher turnover
· Loss of intellectual capital
· Hindered future growth
3. Borrowing Against the Future
Organizations attempt to solve financial problems with debt.
Example:
Hospitals in shrinking communities continue borrowing short-term funds to cover operating expenses, including payroll—because of massive capital projects conceived using arguments from more optimistic times.
Debt postpones the crisis. It rarely solves it.
4. Administrative Expansion
Hospitals merge to improve financial performance but create large administrative structures that increase overhead.
Example:
A group of hospitals forms a system to improve margins, only to spend heavily on corporate headquarters and layers of executive leadership.
Instead of solving financial problems, the merger increases costs and losses in the absence of a solid plan for growing patient volumes and creating net gain efficiencies.
5. The Referral Fantasy
Large tertiary hospitals purchase struggling community hospitals in order to “lock in” referral streams.
But the underlying problems remain:
· Low patient volumes
· Weak community trust
· Operational instability
Without fixing fundamentals, acquisitions simply expand the footprint of dysfunction.
6. The Double Doom Loop
Organizations sometimes attempt to solve complex operational challenges by entering equally complex businesses. Under mounting financial pressure, they pursue risky strategic pivots—often executed quickly, driven more by urgency than by thoughtful planning.
The result is predictable: alienated customers, a confused market position, weakened core fundamentals, and accelerated financial burn.
Example:
A hospital launches its own insurance product, merging two already complex and challenged industries into a single fragile strategy. This internalizes the classic payer–provider tension, where the same organization responsible for improving patient outcomes must also act as the insurer focused on controlling costs and financial risk—often without the operational infrastructure required to balance those competing priorities.
So instead of solving the financial stressors driving the merger, the organization multiplies them in an environment where two struggling systems rarely combine to create one healthy one.
7. Expansion Without Population
In the pursuit of growth, some hospitals expand their physical footprint faster than the population they serve grows. Urgent care centers appear across the region. Clinics multiply. New facilities open with the assumption that greater access will create greater demand, even though market demand remains relatively stable-or at least more stable that the growth would suggest.
Example:
A healthcare system opens multiple urgent care centers and clinics in a region where population growth is limited and competition runs high. Fixed costs—facilities, staffing, equipment, and administrative overhead—rise faster than revenue. Meanwhile, payers continue exercising tighter control over billable services as expansion that was intended to produce growth simply disperses the same patient volume across more buildings and more staff until the math no longer works.
Growth in square footage does not equal growth in demand—or net income.
8. Symbolic Solutions
Organizations under pressure often pursue solutions that signal action rather than generate results. These initiatives are visible. They are easy to announce. They reassure stakeholders that leadership is doing something. But without operational discipline, the initiative never becomes embedded in daily execution. The symbol of action replaces the work of implementation.
Example:
A hospital purchases a mobile outreach bus intended to expand community access and generate new revenue opportunities. A concept that was sound until five years later when the bus had never left the parking lot in the absence of the operational discipline required to turn the idea into a functioning program.
Without discipline, even good ideas become expensive symbols.
9. The Cycle of Repetitive Losses
Organizations that substitute chasing more for operational control often find themselves trapped in a repeating cycle of preventable losses.
• A problem occurs.
• The organization absorbs the loss.
• A lesson is acknowledged.
• But the underlying system that allowed the failure remains unchanged.
The result is predictable: the same problem returns—often larger and more expensive than before.
Example:
A hospital suffers a major cybersecurity breach, incurring more than $3 million in recovery costs, operational disruption, and regulatory exposure. Rather than aggressively strengthening its cybersecurity infrastructure, leadership focused its attention to opening a new clinic to generate additional revenue.
Months later, another breach occurs—rooted in the same vulnerabilities—with even greater losses. Instead of breaking the cycle of repetitive loss through disciplined operational control, the organization attempts to grow its way out of a problem that was entirely preventable.
In the end, whatever the new clinic earns is consumed by preventable losses at the expense of what the operating margin could be.
10. The Illusion of Savings
In the pursuit of growth, healthcare organizations often choose the appearance of savings over the reality of better performance. They hesitate to invest in systems that improve operational control—even when the financial return is clear. The focus remains on generating new revenue rather than strengthening the processes that determine what the profit will ultimately be.
Example:
A hospital considers implementing a structured operational improvement program costing approximately $300,000 per year. Leadership declines the investment, viewing it as a distracting expense. Saving $300,000 on paper while quietly sacrificing what the expected return could be:
First year savings of $1.2–$1.9 million
Reduced operational risk
Improved regulatory control
Freed up caregiver time
Additional long-term savings exceeding $3 million annually through improved efficiency and effectiveness
An illusion of savings that, on face-value, sounds reasonable: preserving capital, avoiding disruption, and concerns about how staff might respond to increased accountability. But the decision reveals a deeper truth. An organization willing to invest millions in new equipment to chase growth—yet hesitates to invest a fraction of that amount to improve how the organization operates.
Sacrificing structural savings for short-term comfort.
11. The Deception of Selective Quality
Organizations that rely on a little quality to promote a reputation for great quality often experience a slow erosion of public trust as decline rarely arrives through a single catastrophic failure. Instead, it emerges quietly—through a gradual weakening of reputation and trust. Each compromising act appears small enough to rationalize, yet is persistent enough to compound.
Example:
A hospital joins one of the many narrowly focused quality initiatives common across the industry. The intent is not to build comprehensive operational control, but to gain marketing advantage. A small set of favorable metrics becomes the foundation for promoting the hospital as a preferred provider.
The CEO, encouraged by a handful of favorable numbers, launches a regional marketing campaign declaring the hospital “one of the safest in the country.” Billboards appear across three counties. For a brief moment, the message works until reality intervenes when the hospital discovers that endoscopic equipment in the operating suite is being improperly cleaned—a failure serious enough to require contacting every patient who underwent the procedure during the previous year.
Public notices appear in newspapers. Radio and television stations share the alerts as patients are urged to seek out testing for potential disease exposure. The billboards that once celebrated safety now frame the crisis as a marketing victory becomes a reputational disaster—costing millions in remediation, legal exposure, lost credibility, and the cancellation of two planned growth projects.
Across the community, the lesson becomes unmistakable: When organizations rely on a little quality to tell a story of great quality, they eventually discover that the gap between the two becomes impossible to hide.
The Pattern Behind the Pattern
These examples may appear different, but they share a common logic. They are all attempts to solve internal problems with external expansion in the absence of the discipline that determines the degree of success. In Collins’ terms, they represent the classic stage of decline where organizations look for silver bullets rather than rebuilding and protecting the fundamentals of their business model. Simple solutions that alone seem inconsequential but in combination feed a drip, drip, drip story of decline. Prioritizing scale instead of quality. Promoting growth without managing execution. Forgetting that in every successful organization, money and quality operate as two sides of the same coin. When one deteriorates, the other eventually follows.
Final Thought
The survival of the healthcare industry depends on its willingness to confront the brutal facts. Today’s leaders and physicians must recognize three fatal mistakes made by their predecessors—and stop repeating them.
Mistake One: The Pursuit of “More.”
Healthcare convinced itself that success could be built through relentless expansion: more services, more technology, more buildings, and more geographic reach.
Mistake Two: Cultural Immunity.
The industry assumed it could operate without consequence inside resistant safety and quality cultures—the kinds described by Philip Hudson and Robert Westrum—where problems are hidden, accountability is weak, learning is slow and patient satisfaction is inconsequential.
Mistake Three: The Shield of Complexity.
Healthcare learned to hide behind the mystique of medicine. Difficult conversations were shut down with technical language and “conversation-stoppers.” Patients were reassured rather than engaged.
Over time, causing patients to adapt. Becoming passive participants in their own care—outwardly compliant and accepting of what healthcare offered but increasingly distrustful. Fearful enough that instead of confronting their providers directly, they turned to regulators, surveyors, and outside authorities to address their dissatisfaction. Resulting is an expanding world of oversight, operational costs that are frequently wasteful, overwhelmed caregivers, and declining public trust.
Bringing healthcare to the defining question: Will it continue chasing expansion while quietly accumulating costs, risks and unhappy patients…. or will it choose what Jim Collins calls renewal and recovery? Discarding the assumptions that have created its problems and embracing the discipline necessary for turning things around.
Recognizing that without balance, growth becomes a liability.